![]()
| Age | 45 years |
| Gender | Male |
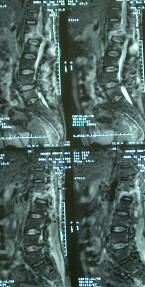
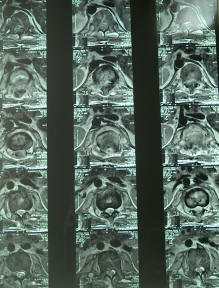
| Diagnosis | Posttraumatic paraplegia at L1 level |
Summary:
The patient was exposed to trauma 3 months ago with subsequent burst fracture of L1 body with paraplegia at that level. The patient was operated elsewhere and fusion was attempted and for unknown reasons the device was removed after 5 days and the patient was left unable even to set down, for the mobile fracture and progressing infection. The patient was treated for 3 months for the infection and was sent to Al-Shmaisani hospital. 28-01-2004, the old incision was refreshed and skeletonization of D10 down to L3 was performed , exposing during that the postganglionic parts of the roots after removal of the intertransverse ligaments above them. Corporectomy of L1 was performed with the aid of drilling. The dura was exposed 3 cm above and below the affected level. The dural sac was seen to be completely transected . Sural nerve grafts were harvested from both legs and a cross anastomosis was performed between the proximal Th11 and L2 distal parts both sides. There was a small piece of sural graft left and used to anastomose the right Th12 with one of the running roots of the cauda equina. After then, using Luque fixation, fusion was performed between D10 down to L3. |




To my knowledge, it is the first operation performed using the postganglionic roots in paraplegia , using sural grafts to improve the regenerating outcome of the neurological state of the patient . From this preliminary experience, it became evident, that there must be at least 10-16 sural grafts to complete the task. It means that there must be nerve graft donor bank to make this mission possible.It is too early to predict the outcome of such procedures, but it is known for more than 100 years that grafts giving results when performed at the postganglionic peripheral nervous system. It is now clear that such procedure can make the paraplegic (walk) , if the lesion is below the mid-dorsal level. This fact will open new dimensions in the surgical treatment of paraplegia. | |
More than 10 months, the surgical activity came to hold, due to lack of donors and the need to promote the idea, for what I have yet no time. For that reason, I strongly appreciate the involvement of other neurosurgeons to make the project come to common practise. Another time, I am not a seeker for authorities or patents.
There are a lot of tasks, which can be achieved, with the creation of nerve graft bank, and many problems waiting to be resolved after then.
24. January 2005 00:33:11
![]()